Table of Contents >> Show >> Hide
- Why This Pandemic Is Often Called “the Greatest”
- 1) It Wasn’t “Just a Bad Flu Season”
- 2) “Spanish Flu” Is a Misleading Name
- 3) Scientists Still Debate the Exact Origin
- 4) The Deadliest Phase Was Not the First Wave
- 5) It Didn’t Mainly Kill Only the Elderly
- 6) Many Deaths Were Linked to Secondary Bacterial Pneumonia
- 7) There Were No Effective Flu Vaccines or Antibiotics in 1918
- 8) Public Health Measures Did MatterEspecially Timing and Layering
- 9) The Pandemic Didn’t Affect Everyone Equally
- 10) It Wasn’t “Forgotten” Because It Was Unimportant
- What the 1918 Pandemic Actually Teaches Us
- Extended Experience Section (Approx. ): What This Pandemic Feels Like in Human Terms
- Conclusion
Let’s address the title first: yes, it sounds like it’s missing the word “wrong.” And honestly, that’s kind of perfect, because the 1918 influenza pandemic (often called the “Spanish flu”) is one of the most misunderstood events in public health history. People still get a lot of things mixed up about ithow it started, who it killed, what worked, what didn’t, and what it actually teaches us today.
This article breaks down 10 facts people still get wrong (or only half-right) about the 1918 pandemic in a clear, readable, SEO-friendly formatwithout turning history into a dry museum placard. We’ll cover the origin debate, the infamous “Spanish” label, why healthy young adults died at shocking rates, why public health timing mattered, and why many deaths were caused by bacterial pneumonia rather than the virus alone. In short: this is pandemic history with context, not folklore.
Why This Pandemic Is Often Called “the Greatest”
When people call the 1918 influenza outbreak the “greatest pandemic in history,” they usually mean one of two things: its extraordinary global reach or its devastating death toll. It infected roughly one-third of the world’s population and killed tens of millions worldwide, with especially severe mortality in the United States and across war-affected regions. If that sounds massive, it was. If it sounds simple, it wasn’t.
With that in mind, here are the facts many people still misunderstand.
1) It Wasn’t “Just a Bad Flu Season”
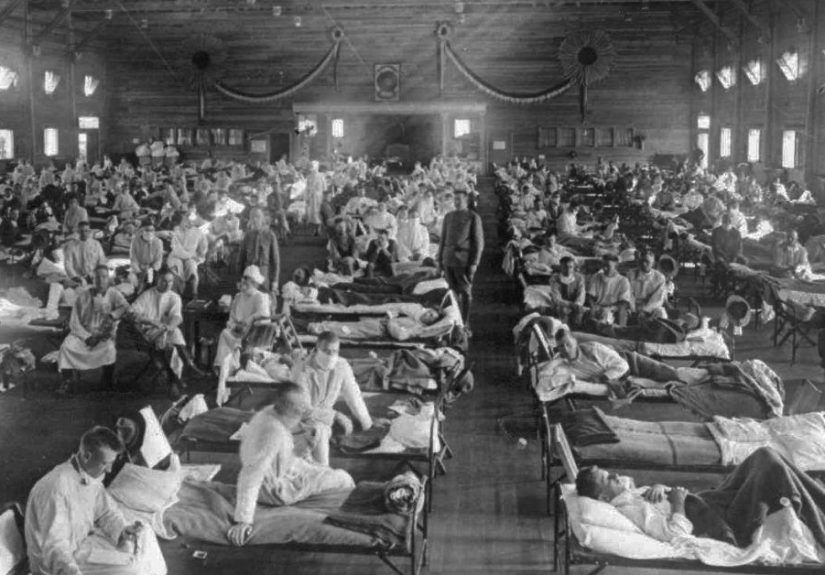
Calling the 1918 pandemic “a really bad flu season” is like calling a hurricane “some wind.” The 1918 H1N1 influenza pandemic was categorically different in scale and severity from ordinary seasonal influenza. It spread rapidly across continents during World War I, infected an estimated 500 million people, and caused mortality levels that transformed demography, public health policy, and medical research for decades.
In the U.S., the impact was so severe that average life expectancy dropped dramatically in a single year. That kind of population-level shock is not what typical seasonal flu does. Seasonal influenza can be serious, but 1918 was a full-blown global catastrophe.
2) “Spanish Flu” Is a Misleading Name
One of the most persistent myths is that the pandemic began in Spain. The name stuck because Spain, unlike many countries fighting in World War I, had a freer press and reported extensively on the outbreak. Other nations were censoring wartime news to avoid hurting morale, so Spain looked like the center of the crisis simply because it was talking about it.
In other words, Spain got branded because it was transparent. Not exactly a great reward for good reporting.
What people still get wrong
Many readers assume the name proves the origin. It doesn’t. “Spanish flu” is better understood as a historical nickname created by information imbalance, not a scientific conclusion.
3) Scientists Still Debate the Exact Origin
A lot of people speak about the pandemic’s origin with absolute certainty. History is not that neat. While Kansas (especially Camp Funston/Fort Riley and the broader Haskell County hypothesis) is one of the strongest and most discussed origin theories in U.S.-based scholarship, researchers have also examined alternative hypotheses involving Europe and Asia.
The key point: the origin story remains debated because data from that era were incomplete, virology was still primitive, and wartime conditions complicated surveillance. So if someone says, “It definitely started here and case closed,” that confidence may be higher than the evidence supports.
4) The Deadliest Phase Was Not the First Wave
Another common misconception is that the pandemic hit once and simply burned through the population in a single giant surge. In reality, the 1918 pandemic unfolded in multiple waves. The early wave in spring 1918 was generally milder in many places, while the fall waveespecially between September and November 1918 in the U.S.was dramatically more lethal and accounted for most deaths.
This matters because it explains why some communities felt they had “survived” the pandemic, only to be devastated later. It also explains why public health officials who delayed action in the fall wave paid a terrible price in mortality.
Why this still matters
Pandemics are not always one-and-done events. People often relax too early after an initial decline, assuming the danger has passed. History suggests that second and later waves can be worse.
5) It Didn’t Mainly Kill Only the Elderly
Seasonal influenza usually hits the youngest and oldest populations hardest. The 1918 pandemic broke that pattern in a shocking way: healthy young adultsespecially people in their 20s, 30s, and early 40sdied in unusually high numbers. That “W-shaped” mortality pattern is one of the most famous and puzzling epidemiologic features of the pandemic.
This is one reason the outbreak terrified communities. When a disease disproportionately kills grandparents, people panic. When it kills young adults in their primeworkers, soldiers, parents, nurses, teacherssociety starts to feel structurally unstable. The 1918 pandemic did both.
6) Many Deaths Were Linked to Secondary Bacterial Pneumonia
One of the biggest facts people still miss is that many 1918 deaths were not caused by the influenza virus alone. A large share of fatalities appear to have involved secondary bacterial pneumonia. The influenza infection damaged the respiratory tract, and common bacteriaespecially pneumococci, streptococci, and staphylococciwere then able to cause severe, often fatal complications.
This detail is more than medical trivia. It changes how we understand both the history and preparedness lessons. The 1918 disaster was not only a story about viral transmission; it was also a story about bacterial coinfections, crowding, and the limits of medical treatment at the time.
Translation into plain English
The virus kicked the door open. Bacteria barged in and did enormous damage.
7) There Were No Effective Flu Vaccines or Antibiotics in 1918
It’s easy to accidentally project modern medicine backward. People assume doctors in 1918 had the same toolkit we do nowjust less polished. Not even close. Influenza viruses had not yet been identified as they would be in the 1930s, and the first widely available influenza vaccines came later (with major advances in the 1940s). Antibiotics, which would later transform bacterial pneumonia treatment, were not available in 1918.
That means doctors and nurses faced a fast-moving, highly lethal respiratory pandemic with limited diagnostic tools and no effective antiviral drugs, no modern ventilators, and no antibiotics for many fatal secondary infections. Public health measures were not a “backup plan” in 1918they were the plan.
8) Public Health Measures Did MatterEspecially Timing and Layering
Another myth is that city-level interventions were pointless because “everyone got it anyway.” Historical analyses of U.S. cities show a more nuanced reality: communities that acted earlier and used layered nonpharmaceutical interventions (NPIs)such as closing schools, canceling public gatherings, and isolating casesoften reduced peak mortality and slowed transmission.
The famous Philadelphia vs. St. Louis comparison illustrates this. Philadelphia allowed a massive Liberty Loan parade despite warnings; the city experienced a catastrophic surge soon afterward. St. Louis, by contrast, moved earlier to restrict crowds and is widely cited as having a flatter epidemic curve. This wasn’t magic, and it wasn’t perfect. But timing mattered. A lot.
Important nuance
NPIs did not make cities invincible. Some places still faced later waves, social pushback, and uneven compliance. But early, sustained, layered action was associated with better outcomes than delayed or fragmented responses.
9) The Pandemic Didn’t Affect Everyone Equally
People sometimes describe the 1918 pandemic as a “great equalizer.” It wasn’t. While the virus spread broadly, outcomes were shaped by crowding, poverty, wartime movement, access to care, and local infrastructure. Military camps, ships, and densely populated cities became accelerators. Communities with fewer resources often faced worse outcomes.
In the United States, some Native and Alaska Native communities suffered devastating mortality. Historical records also show severe strain in places with nursing shortages and overwhelmed hospitals. A virus may be biologically opportunistic, but its damage is often socially patterned. The 1918 pandemic made that brutally clear.
10) It Wasn’t “Forgotten” Because It Was Unimportant
People are often surprised by how little they learned about the 1918 pandemic in school. That leads to a strange assumption: if it was so catastrophic, why doesn’t it dominate historical memory? The answer is not that it lacked importance. It’s that it overlapped with World War I, was fragmented across local experiences, and often left behind records of grief rather than a single clean political storyline.
In some historical narratives, war got the monuments and influenza got the death certificates. But public health history, archival collections, and modern scholarship have steadily restored the pandemic to its rightful place as one of the defining disasters of the modern era.
What the 1918 Pandemic Actually Teaches Us
If there’s one lesson from the greatest pandemic in history people still get wrong, it’s this: pandemics are never only about pathogens. They are also about communication, timing, institutions, trust, inequity, and whether a society can act before the morgues are full.
The 1918 influenza pandemic teaches us that names can mislead, data can be incomplete, medical certainty can arrive late, and public health decisions often have to be made under uncertainty. It also teaches us that basic interventionsboring, disruptive, politically unpopular interventionscan buy time and save lives.
History doesn’t repeat itself in a copy-paste way. But it does rhyme, and sometimes it rhymes in a cough.
Extended Experience Section (Approx. ): What This Pandemic Feels Like in Human Terms
One reason people still misunderstand the 1918 pandemic is that they treat it as a chart instead of an experience. But the story of the greatest pandemic in history is not only numbers on a page. It is also the experience of confusion, mixed messaging, exhausted caregivers, and ordinary people trying to decide whether to keep living normally or change everything overnight.
Imagine hearing that there is “some influenza” going around, then watching your town move from mild concern to full crisis in a matter of days. That transitionwhen the familiar becomes frighteningis one of the most important human experiences tied to pandemics. In many communities in 1918, life did not look apocalyptic until suddenly it did. A parade happened. A train arrived. A camp outbreak spread. Then hospitals overflowed, nurses were in short supply, and people realized too late that the situation was not routine.
Another deeply human experience is the mismatch between personal observation and public reality. If your household is healthy, the warnings can feel exaggerated. If your block is grieving, they feel too weak. That tension still shapes how people respond to outbreaks: some want stronger action immediately, others want proof visible from their own front porch. The 1918 pandemic shows how dangerous that gap can be, especially when disease growth is exponential and officials wait for certainty instead of acting on early signals.
Caregiving is another underappreciated experience. Historical accounts repeatedly point to overworked nurses, volunteers, families, and neighbors filling the gaps when systems failed. In practical terms, pandemics become local long before they are “historic.” Someone has to bring food, check on the sick, wash linens, mind children, bury the dead, and keep basic services running. The emotional burden of that work rarely appears in summary timelines, but it is central to understanding what large-scale disease actually does to a society.
There is also the experience of stigma and language. A misleading disease name can shape public fear and blame, turning a health emergency into a story about outsiders rather than transmission dynamics. That emotional shortcut may feel satisfying, but it is terrible public health. The 1918 “Spanish flu” label is a classic example: a name tied to reporting patterns became a false origin story, and the false story outlived the emergency.
Finally, there is the experience of forgetting. Many families remembered 1918 privately while institutions under-taught it publicly. That creates a strange historical echo: each generation feels like it is encountering pandemic uncertainty for the first time. Revisiting these facts is not about nostalgia or panic. It is about building memory strong enough to resist myth. The 1918 pandemic still matters because the human experiences around itdenial, courage, fatigue, improvisation, grief, and solidarityare exactly the experiences that shape how societies survive the next crisis.
Conclusion
The 1918 influenza pandemic remains one of the most important case studies in public health, epidemiology, and social response. It was devastating not only because of the virus itself, but also because of wartime conditions, delayed interventions, limited medical tools, secondary bacterial infections, and uneven systems of care. If you want the clearest takeaway, it’s this: the facts matter, and the details matter even more.
Understanding the greatest pandemic in history means moving beyond the nickname, beyond the myths, and beyond the oversimplified “people panicked” narrative. The real story is richer, stranger, and more usefuland yes, still painfully relevant.